
 FP1032 : Management of anterior corneal scars: T-FALK is the way ahead
FP1032 : Management of anterior corneal scars: T-FALK is the way aheadDr. VIJAY KUMAR SHARMA
Dr. ALOK SATI
Semi Finals
Abstract
Aim: To report a modified suture-less and glue-less technique, termed as tuck in femtosecond laser assisted anterior lamellar keratoplasty (T-FALK), to achieve a good graft host junction apposition.
Methodology: A prospective interventional case series of fifteen eyes of fifteen patients, who underwent T-FALK.
Results: A total of fifteen patients (08 males and 07 females) underwent T-FALK. Six patients had superficial corneal opacities post healed microbial keratitis, 05 patients had spheroidal corneal degeneration, 03 had Salzman nodular degeneration and one patient had vortex keratopathy. No intraoperative or postoperative complications were noted during the T-FALK. All patients had good graft host junction apposition postoperatively as demonstrated by ASOCT.
Conclusion: Suture-less and glue-less T-FALK can be the best way ahead for management of superficial anterior corneal scars with good visual outcome.
Full Text
Management of anterior corneal scars: T-FALK is the way ahead
Col Vijay K Sharma, Col Alok Sati
Army Hospital R&R Delhi
Sutureless anterior lamellar keratoplasty (SALK) is a lamellar corneal transplantation procedure for the treatment of corneal scars, limited to anterior 150-200 microns of cornea. SALK provides advantages of sutureless lamellar corneal surgery procedure to treat anterior corneal opacities. It can be performed-either by using microkeratome where a particular thickness blade is used for cutting donor and recipient lamellar corneal buttons or by using femtosecond laser for programmed cutting of donor and recipient partial thickness corneal tissues as in femtosecond laser assisted sutureless anterior lamellar keratoplasty (FALK). One of the major concerns for ophthalmologists while performing SALK is sizing of appropriate donor and recipient cuts for achieving good apposition of graft host junction. We describe a modified sutureless and glueless technique termed as ‘tuck in’ femtosecond laser assisted sutureless anterior lamellar keratoplasty (T-FALK) for management of anterior corneal scars.
Methodology
A total of fifteen eyes of fifteen patients with anterior corneal opacities, involving anterior 200 microns of cornea underwent T-FALK. T-FALK was performed using VISUMAX femtosecond workstation (Carl Zeiss Meditec AG, Jena, Germany). Initially, donor cornea was mounted over artificial anterior chamber and epithelium was removed by scraping. Based on depth of corneal opacity, as measured by ASOCT, parameters were fed in to the Visumax femtosecond workstation to cut similar thickness and diameter as was planned for host lamellar surgery. Femtosecond parameters used included energy setting of 36 with single spiral out scan direction with a track distance of 4.5 microns, spot distance of 4.5 microns and side cut angle of 45 degrees instead of conventional 90 degrees used in previous studies. Then recipient lamella was cut using similar parameters. No oversizing of donor tissue by 0.1mm was done as was suggested in earlier studies.8,9 Depth of donor lamellar cut was kept 10% more compared to recipient lamellar cut to cater for any swelling in the cornisol preserved donor tissue. The epithelium was removed in donor corneas where epithelium was edematous or had epithelial defects, to achieve a uniform plane of dissection with femtosecond laser. Diameters of donor and recipient lenticules were kept similar and between 7.9 to 8.5mm. All procedures were done under topical anesthesia using proparacaine hydrochloride 0.05% eye drops. After cutting donor and host tissues, donor tissue was transferred to the recipient bed. After aligning the donor tissue over the recipient bed, edges of the donor graft were tucked under the host corneal margins all around 360 degrees as created by 45 degrees femtosecond side cut. A bandage contact lens (BCL) was applied at the end of the procedure. Eye drop moxifloxacin hydrochloride 0.5% was instilled after the procedure. All patients were advised eye drop prednisolone sodium phosphate 1% four times a day and eye drop moxifloxacin hydrochloride 0.5% four times a day for next three weeks. BCL was removed after three weeks. UCVA, BCVA and slit lamp biomicroscopic evaluation was done at each follow up visit. ASOCT was done to assess the healing and apposition of the graft at one day, one month and three months. Eye drop moxifloxacin hydrochloride 0.5% was stopped after three weeks. Eye drop prednisolone sodium phosphate 1% was tapered to three times a day for next two weeks and twice a day for next two months.
Results
A total of 15 patients (8 males and 7 females) underwent T-FALK using VISUMAX femtosecond workstation. Six patients had superficial corneal opacities following healed microbial keratitis, 5 patients had spheroidal corneal degeneration, 3 had Salzmann nodular degeneration and 1 patient had vortex keratopathy. The mean preoperative depth of corneal scar was 148 ± 9.4 microns and mean thickness of recipient scarred lenticule removed was 153.3 ± 9.0 microns. Mean thickness of donor lenticule was 168.7 ± 9.9 microns which reduced to 153.2 ± 8.8 microns, three months postoperatively as measured by ASOCT. Mean preoperative BCVA was 0.96 ± 0.093 logMAR units which improved to 0.53 ± 0.057 logMAR units three months after the procedure. The p value was 0.0006 and was highly significant. Postoperatively, refraction was possible in all patients suggesting clearing of visual axis and decrease in irregular astigmatism. Four patients where refraction was possible preoperatively, showed mild hyperopic shift in the spherical error (1.37D preoperatively to 1.5D postoperatively at three months) and decrease in astigmatism from preoperative mean value of 1.63D to 0.47D, 3 months postoperatively. Fig 1
Discussion
Femtosecond assisted-shaped corneal transplantation procedures are being increasingly performed due to availability of precise femtosecond laser cutting technology with ability to design full thickness as well as lamellar grafts with respect to margin or overall diameter. FALK offers many advantages over conventional microkeratome assisted SALK. It can be programmed for any precise depth or diameter of lenticule cut as opposed to microkeratome which has limitation of fixed diameter and depth. The graft host junction apposition in post SALK patient is variable and is theoretically considered to be better in FALK, compared to microkeratome assisted SALK.
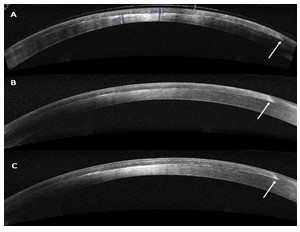
In T-FALK, we have modified side cut angle to 45 degrees for both donor and recipient cut, keeping overall diameter same for both. When donor lenticule is placed on recipient bed, margins of the donor lenticule can be tucked under the recipient cornea providing overlap varying from 150 to 400 microns between two lamellar margins, depending upon the thickness of femtosecond lamellar cut. While on one aspect, it provides more surface area between two lamellar marginal surfaces to heal, it also covers for small mismatch between the donor or recipient lenticule size. There is no uneven surface as donor and host tissue are similar in overall diameter and side cut thus, providing better apposition and healing at graft host junction. Fig 2
As shaped corneal transplantation surgery is, probably, the way ahead for corneal transplantation procedures despite being technologically challenging and concerns of cost-effectiveness, suture-less and glue-less T-FALK may lead to further improvement in biomechanics at graft host junction following lamellar corneal transplantation for management of anterior corneal scars.
Fig 1
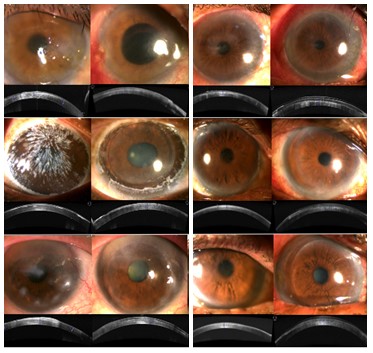
Fig 2
Leave a Comment