

 FP1836 : National Survey for mapping Human Resource & Infrastructure for Eye Care Services in India
FP1836 : National Survey for mapping Human Resource & Infrastructure for Eye Care Services in IndiaDr. PRAVEEN VASHIST
Dr. SURAJ SINGH SENJAM, Dr.Vivek Gupta, Dr. ROHIT SAXENA
Semi Finals
Abstract
An ongoing nation-wide survey for mapping of current human resource and infrastructure for eye care in India. A database of 10,964 probable eye care institutes in India was prepared. These institutes were requested telephonically to participate in an online survey. 6,990 institutes (63.8%) have been contacted so far and of these 5415 (77.5%) reported having secondary or tertiary level eye care facilities. An interim analysis of the data received from 2102 institutes revealed a total of 5744 full time ophthalmologists (mean 2.7) and 7493 optometrists (mean 3.6). An average of 20,178 patients were seen and 1840 surgeries done at each centre in last one year. Detailed information was collected for pediatric ophthalmology services. 739 institutes reported of having paediatric ophthalmology services with an average of 103 paediatric surgeries done in last one year. The data will be incorporated in India vision atlas as real-time online public access to benefit the policy-makers.
Full Text
National Survey on Human Resources and Infrastructure for Eye Care Services in India
Abstract: The year 2020 marks the final year for the achievement of targets of the Vision 2020 Right to Sight initiative. The objectives of the study were to determine the human resources and infrastructure available for ophthalmic services, including paediatric services, in secondary and tertiary level hospitals in India, and to determine the achievement of targets related to human resources and infrastructure as per Vision 2020 Right to Sight norms. An online questionnaire was mailed to all eye-institutes of the country and telephonic follow up was done to ensure response. A total of 9440 eye institutes were identified in the country through various yellow pages and available online directories, which were requested for participation in the survey. Out of them, 8790 (93.1%) institutes were contacted telephonically, and remaining institutes could not be contacted. Of 8790 eye-care institutes, a complete response was obtained from 7901 institutes (response rate 89.9%) and among them 2180 institutes (27.6%) reported to have pediatric eye care services. The number of optometrists per ophthalmologist was 0.85 whereas the ophthalmologist population ratio was found to be 1: 65221 in the country. One encouraging finding of the survey was 8 paediatric ophthalmologists per 10 million population which is a much more optimistic figure than the minimum requirement of 1 per 10 million.
Introduction
The elimination of avoidable blindness is the major goal of the World Health Organization (WHO) and the national governments in different countries.[1] The Vision 2020 – Right to Sight initiative is committed to strive for the elimination of major causes of avoidable blindness globally.[2] Childhood blindness is areas of concern of all national and international efforts especially in developing countries like India. [3] Half of childhood blindness load is amenable to current preventive and curative strategies. In such a situation, it is important to provide comprehensive eye care services to tackle childhood blindness across the country. The WHO estimates that in 2015 there were 253 million people with visual impairment, including 36 million people blind globally.[4] Though the overall prevalence of blindness and visual impairment is much lower in children compared to adults, children need overarching attention because of the number of years that they would live with blindness or impaired vision. The global estimate of children with severe visual impairment and blindness (SVI/BL) is 1.4 million,[5] of whom nearly 300,000 are in India.[6]
Causes of childhood blindness have been estimated from two sources in India. One set of estimates is derived from studies done on children in schools for the blind while the other set is based on population-based studies. Retina, cornea and whole globe have been reported to be the commonest anatomical site for blindness in children in institutional studies,[7] while refractive error and amblyopia were reported to be the commonest causes in population-based studies.[8]
In the Vision 2020 Action plan, Government of India targets to train 200 ophthalmologists, pediatricians, anesthetists and paramedics in various fields related to paediatric ophthalmology to combat childhood blindness in India.[9] By the year 2020, the Government of India visualizes the development of paediatric ophthalmology units at all tertiary health care institutions. It was aimed to provide specially trained paediatric eye care personnel at centers established at the norm of 1 per 10 million population.[10]
There is a paucity of data on the availability of services as well as infrastructure to tackle childhood blindness, especially in the public sector. A few studies were conducted more than a decade ago and data was collected from medical colleges and NGO eye hospitals on the infrastructure and human resources for paediatric eye care.[11,12]
Planning effective eye care service delivery systems for children needs baseline data on the availability of eye care services for control of childhood blindness and visual impairment at the tertiary and secondary level. It is also required to obtain the estimates of what proportion of ophthalmologists are currently engaged in providing eye care services to children.
The availability and deployment of trained human resources and the establishment and adequate functionality of available infrastructure are both important for the control of childhood blindness and visual impairment. The objectives of the study were to determine the human resources and infrastructure available for providing ophthalmic services from the existing secondary and tertiary level hospitals in India and to assess the achievement of targets related to human resources and infrastructure as per Vision 2020 Right to Sight norms.
Methodology:
Study Setting: India is a union of 28 states and 9 union territories, having a total of 739 districts. The study was undertaken over one year period from January 2020 to December 2020.
Development of study questionnaire: Previous surveys on eye care services were studied and subjected to extensive discussion and scrutiny by the investigators. This period included January 2020 to March 2020 during which time an extensive phase of qualitative discussions was done to suggest data collection strategies that fit the national context, to verify that all definitions were understood and to investigate internal data discrepancies and non-response fields. Inputs were also obtained from Non-Governmental Organization partners, National Program for Control of Blindness, Government of India, All India Ophthalmic Society and Vision 2020- The Right to Sight India. For the present survey, it was decided to include institutes having at least one ophthalmologist. Hence, vision centres manned by Ophthalmic Assistants were not included in the survey. VISION 2020- The Right to Sight India, targets were used as a benchmark for data on HR while the equipment were selected by a team of expert from the International Agency for Blindness and Prevention list of equipment. [13–15] The ethical permission for conducting the study was obtained from the Institute Ethics Committee of All India Institute of Medical Sciences New Delhi.
Data were collected in two phases using different strategies as follows:
(i) An online questionnaire-based survey, including paediatric eye facilities using a specially developed questionnaire on Human Resources, Infrastructure, and Equipment (ii) Online meetings with SPOs (State Program Officers) and DPOs (District Program Officers) in all states/UTs.
For the first phase of data collection, a list of eye care facilities including their physical addresses, telephone numbers and email IDs were first prepared by searching yellow pages and available online directories. Online search was performed using NIC (National Informatics Centre) district portals, Ayushman Bharat Directories along with websites of reputed private hospitals. AIOS (All India Ophthalmological Society) database of ophthalmologists was used to find names and contact details of ophthalmologists in districts. The list was supplemented with information from eye care personnel who knew of other facilities not captured in the initial list. Private-for-profit and non-profit eye care facilities were also included in the search.
Once the baseline database was completed, the survey questionnaire was emailed to respective eye-care facilities for self-completion followed by a preliminary contact via email, telephone calls, or text messaging. In addition, a link to an online version of the questionnaire, created using Monkey Survey©, was sent by text messaging or email to the representatives of the facilities. Reminders were sent via telephone calls or text messaging to maximize responses. Data collected included background information on the facility like name, address and head of the department, sub-specialities available, human resource
for eye health and paediatric eye-care, and equipment details. An institute was assumed to be providing paediatric ophthalmology services only if it provided surgical paediatric eye care with availability of general anaesthesia facility. For such institutes, detailed information about paediatric ophthalmology services was obtained including diagnostic, out-patient, in-patient and surgical services. Duplicate data were removed promptly and incompletely filled forms were completed telephonically.
The second phase of the data collection started from July 2020 and was completed by December 2020. Representatives from NPCB&VI, Government of India was requested to issue a letter to all SPOs and DPOs informing them about the survey and soliciting their co-operation for the same. Starting from July 7, 2020, online orientation meetings were conducted with each state in which the respective SPO along with DPOs from all districts were invited. During these video-conferencing meetings, the questionnaire was explained in details and status of data collection was presented till the date of meeting. Opportunity was utilized to solve any queries regarding the questionnaire raised by the DPOs. Following the meet, email IDs and contact details of all DPOs was obtained from the SPO and district-wise database of eye institutes was emailed to each of them.
In each district, DPOs were telephonically requested to coordinate data collection and updating. DPOs also identified the other key informants/responsible persons from government/NGO or private section to collect information on human resource and infrastructure as per the questionnaire. For each state, Dr. Rajendra Prasad Centre for Ophthalmic Sciences recruited Coordinators from Community Ophthalmology section. These coordinators were encouraged to use several sources of data including SPO/DPOs, professional networks (ophthalmologists and optometrists’ associations), medical colleges and eye care non-governmental organizations (NGOs). A separate What’s app group was formed in each state to resolve day-to-day queries. The daily reporting status was shared among the group members. Once the database was finalized in each district, efforts were made to obtain completed forms from each of the eye institute in that particular district.
Quality assurance: In order to increase the validity of the data collected, triangulation method was used. The data obtained from each institute was emailed back to the head of the institute for confirmation and necessary rectification. This acknowledgement mail also ensured that the head of the department was aware of regarding the response received from their institute, so that any future rectification or updating can be done easily in the future.
Data management and analysis
For consistency, all data was reviewed by a single researcher as it was received, to identify inconsistencies and likely reporting errors in the data requiring follow-up. Data that was received offline was entered directly into a Stata 15.0 (StataCorp, College Station, TX, USA) database and cross-checked for avoiding duplication. Stata 15.0 was used for all statistical analyses.
Results
A total of 9440 eye institutes was identified after intensive online searched from the country. Out of them, 8790 (93.1%) institutes were contacted telephonically, and remaining institutes could not be contacted owing to lack of correct contact details. Out of the 8790 eye-care institutes in the country, complete responses were received from 7901 institutes (response rate 89.9%) and 2180 institutes (27.6%) reported to have paediatric eye care services. (Table 1, Figure 1)
Infrastructure and HR: states
The states contributing to the highest proportion of eye-institutes in the country include Maharashtra (17.2%), Uttar Pradesh (9.1%), Gujarat (8.2%) & Karnataka (6.4%). These four states along with Tamil Nadu, Andhra Pradesh, Telangana, Rajasthan & West Bengal constitute nearly two-thirds (67.7%) of all eye-care institutes in the country. On the other hand, states like Madhya Pradesh (3.1%), Bihar (3.1%) & Odisha (2.2%) have the lowest proportion of eye-care institutes in the country.
Out of the 7901 eye-care institutes in the country, 2180 (27.6%) of them were found to have paediatric oriented services.
The states contributing to the highest proportion of paediatric eye-institutes in the country include Maharashtra (22.6%), Gujarat (9.4%), Uttar Pradesh (8.9%) & Karnataka (5.8%). These four states along with Haryana, Punjab, Tamil Nadu & Rajasthan constitute nearly two-thirds (67.8%) of all paediatric eye-care institutes in the country. On the other hand, states like Himachal Pradesh (0.6%), Assam (1.2%), Odisha (1.2%) & Chattisgarh (1.3%) have the least number of paediatric institutes in the country.
As far as the proportion of institutes having paediatric oriented services is concerned, the highest proportion was found in states like Punjab (36.4%), Maharashtra (36.2%) & Haryana (36.2%). At the other end of the spectrum are states like Goa, Telangana, Sikkim, Arunachal Pradesh & Odisha where less one sixth of all eye institutes had paediatric oriented services.
Among the 9 union territories, the highest proportion of eye-institutes was found in Delhi (3.2%), including the NCR (National Capital Region). The highest proportion of paediatric eye-institutes was also found in Delhi (5.0%) followed by Chandigarh (0.5%). UTs which did not have even one paediatric eye institute are Daman & Diu & Lakshadweep. The proportion of total eye institutes having paediatric oriented services was highest in Chandigarh (47.6%), closely followed by Delhi (43.8%). (Table 2)
Infrastructures and HR: National
As far as ownership of eye-institutes is concerned, nearly 2/3rd of institutes (70.6%) was in the private sector, followed by public sector (15.6%) and NGO sectors (13.8%). The number of optometrists per ophthalmologist at secondary / tertiary levels was 0.85. The ophthalmologist population ratio in the country was found to be 1: 65221 and the optometrist population ratio was 1:76530. Number of eye-beds per million population was 74. Proportion of eye institutes having 24 hours eye emergency was 40.5%, while functional eye OT was reported by 87.0% of institutes. Facility of eye bank (with tissue processing & storage) was reported by only 5.7% of the institutes. Refractive eye surgery was reported by 20.9% of institutes, whereas low vision services were reported by 28.3% of institutes. Most common sub-speciality services include cataract (91.5%), glaucoma (71.5%), squint (42.0%), oculoplasty (37.3%) and vitreo-retina (33.6%). Neuro-ophthalmology services were reported by only 25.4% of the institutes, whereas keratoplasty services were reported by only 14.4% of the institutes. (Table 3)
The proportion of institutes having 24 hours eye emergency, functional eye OT, eye bank (with tissue processing facility), refractive eye surgery & low vision services was reported significantly higher in the private sector in comparison to the public sector and NGO sector. (Table 4). Similarly, the proportion of institutes having sub-specialities of cataract, glaucoma, squint, uvea & vitreo-retina, keratoplasty, oculoplasty & neuro-ophthalmology was reported significantly higher in the private sector in comparison to the NGO sector and public sector. (Table 5)
Out of the 2180 institutes reported of facilities of paediatric surgery under general anaesthesia, 71.3% were in the private sector, followed by NGO (17.2%) and public sectors (11.5%); and this difference was statistically significant. Paediatrician to handle cases were available in 1604 (73.5%) of the institutes & anaesthetists to handle paediatric cases were present in all institutes. Only 142 (6.5%) of the institutes were training institutes, providing formal training in the form of fellowship or senior residency in paediatric ophthalmology, and 45.8% of them were in private sector closely followed by the NGO sector (42.3%). Paediatric ophthalmology outpatient services (OPD) were present in 1795 (82.3%) of the institutes & overnight admission facilities were present in 1206 (55.3%). (Table 6)
The availability of paediatric equipment was also highest in the private sector, followed by NGO sector & public sector. (Table 7)
As per the current survey, there are around 16 paediatric eye-care institutes per 10 million population in the country, and the number of paediatric ophthalmologist (having received formal training or fellowship in paediatric ophthalmology) per 10 million was 8. The average eye OPD per million population was 83008 for general ophthalmology, which includes 4376 of paediatric (up to 18 years) patients. Similarly, the average eye surgery per million population was 6178 for general ophthalmology, which includes 112 of paediatric (up to 18 years) patients. Out of 100 paediatric eye institutes, average of 6-7 provide formal training (fellowship or senior residency) in paediatric ophthalmology. (Table 8)
On an average, there are 74 eye beds per million population, out of which only 3 beds are dedicated to paediatric patients. The proportion of total eye operations that were performed on paediatric patients was 1.8%. Among the paediatric surgeries, the highest proportion was for cataract (34.1%), followed by other adnexal operations (29.1%) and squint (17.7%). The proportion of glaucoma surgeries was 3.9%, oculoplasty/oncology was 9.3% and keratoplasty 1.6%. (Table 8) Out of total paediatric OPD, proportion of ROP screening was 5.3%. Out of all the children screened, LASER was performed on 8.3% of the patients. The proportion of ROP surgery among all paediatric surgeries was 4.3%. (Table 9)
A list of 14 equipment was used in the survey to assess the infrastructure for providing paediatric eye care; the instruments were divided into those required for OPD & those required for surgery. Proportion of paediatric eye institutes having functional retinoscope was 97.6% indirect ophthalmoscope 97.3%, trial sets 95.0%, prisms for squint assessment 82.4%, handheld tonometer 79.7% and other tonometer 88.7%. Pre-verbal vision test (Teller’s/Cardiff VA Card) was available with only 61.1% of the eye institutes, whereas RetCam/Paediatric fundus camera was available with only 28.9% of institutes. (Table 10)
Similarly, proportion of paediatric eye institutes having functional operating microscope was 98.6% A-scan ultrasound 96.0%, keratometer 95.2% and phaco machine 94.7%. Vitrectomy machine was available with 74.6% of institutes, whereas ROP laser was available with only 49.1% of institutes. (Table 10)
Discussion
A child becomes bilaterally blind every minute, primarily within developing nations. Such children need to be addressed to achieve the goal of Vision 2020- The Right to Sight. The number of optometrists per ophthalmologist at secondary / tertiary levels in the current study was 0.85 in the current study. Ideally the ratio of paramedics should be 3 to 4 per ophthalmologist. Although the target year 2020 has already arrived, there is still a long way to go to achieve adequate number of ophthalmic paramedics in the country. The ophthalmologist population ratio in the country was found to be 1: 65221. Again, the target for ophthalmologists was to achieve a ratio of 1:50000 with at least 25000 trained ophthalmologists by 2020. The number of ophthalmologists in the current survey was 20944. Even if we add 10% to this number due to non-response by institutes, it still falls short of the 25000 required to achieve in the country by 2020. One encouraging finding of the survey was 8 paediatric ophthalmologists per 10 million population which is a much more optimistic figure than the minimum requirement of 1 per 10 million.
There has been no formal training for paediatric ophthalmology till recently, although paediatric ophthalmology departments are now being set up in tertiary care eye hospitals. Such departments do not cater only to children but provide services across all age groups. Only recently have institutions like Aravind Eye Care System, Sankara Netralaya and L.V. Prasad Eye Institute, which have been labelled as paediatric ophthalmology learning and training centres, have formalized fellowship programs in paediatric ophthalmology. More ophthalmologists are now opting for paediatric ophthalmology fellowship training.
Though paediatric ophthalmology is now developing as a distinct subspecialty in India, the clinical load may not warrant a situation in most hospitals of specialty ophthalmologists working only in paediatric ophthalmology. To attract ophthalmologists to take up paediatric ophthalmology, it would be necessary to allow them to also attend to ophthalmic problems in other age groups to generate adequate professionally satisfying workloads.[12]
Though a significant number of hospitals in the country have either specialty trained or oriented ophthalmologists, they are usually not supported by a trained paediatric team, as was observed in the present study. The subspecialty needs a team approach to be successful and identifying modalities of training a composite team of ophthalmologists, optometrists, nurses, anaesthesiologist and counsellors needs to be addressed. The WHO also strongly recommends the team approach.[10]
The present study was one of its kind in the Indian subcontinent to collect information on the status of paediatric eye care services. The WHO suggests that there should be one paediatric ophthalmology service centre for every 10 million population, where at least one specialty trained or oriented ophthalmologist should be available. There were 2180 such centres for a population of 1.3 billion, translating to 8 paediatric ophthalmology service units per 10 million population. Many of these hospitals do not have a full complement of diagnostic and surgical equipment, infrastructure and supportive human resources to provide vibrant paediatric ophthalmology services. The available centres are also not homogenously distributed across the country. Better ratios were observed in the southern and western part of India as against thin distribution of services in the North and East. Paediatric eye care services need further strengthening via investment of time and money, and a professional and political commitment is required to support the establishment of need-based paediatric centres.
Bibliography
- World Health Organization. Elimination of avoidable blindness. World Heal Organ 2003;(April):2003–6.
- Louis Pizzarello, Abiose A, Ffytche T, Duerksen R, Thulasiraj, Taylor H, et al. Vision 2020: The Right to Sight- A Global Initiative to Eliminate Avoidable Blindness. Arch Ophthalmol 2004;122(April):615–20.
- Wadhwani M, Vashist P, Singh SS, Gupta V, Gupta N, Saxena R. Prevalence and causes of childhood blindness in India: A systematic review. Indian J Ophthalmol 2020;68(2):311–5.
- Bourne RRA, Flaxman SR, Braithwaite T, Cicinelli M V, Das A, Jonas JB, et al. Magnitude, temporal trends, and projections of the global prevalence of blindness and distance and near vision impairment: a systematic review and meta-analysis. Lancet Glob Heal 2017;5(9):e888–97.
- Dandona R, Dandona L, Srinivas M, Sahare P, Narsaiah S, Muñoz SR, et al. Refractive error in children in a rural population in India. Invest Ophthalmol Vis Sci 2002;43(3):615–22.
- Agarwal P, Maan V, Omaer M, Gupta K, Chauhan L, Khurana A. Clinical profile of childhood blindness and inappropriate enrolment of children in schools for visually impaired in Uttar Pradesh, India. Indian J Ophthalmol 2018;66:1456–61.
- Titiyal JS, Pal N, Murthy GVS, Gupta SK, Tandon R, Vajpayee RB, et al. Causes and temporal trends of blindness and severe visual impairment in children in schools for the blind in North India. Br J Ophthalmol 2003;87(8):941–5.
- Dandona R, Dandona L. Childhood blindness in India: a population based perspective. Br J Ophthalmol 2003;87(3):263–5.
- Vision 2020: The Right to Sight-India. The global initiative for the elimination of avoidable blindness: Action Plan 2006-11. World Heal. Organ.1998;11(26):2.
- World Health Organization (WHO). A five-year project for the prevention of childhood blindness. 2002;
- Murthy G, Malhotra S. Status of Eye Care in South East Asia Region. Delhi J Ophthalmol 2013;24(2):114–8.
- Murthy G, John N, Gupta SK, Vashist P, Rao G V. Status of paediatric eye care in India. Indian J Ophthalmol 2008;56(6):481–8.
- International Agency for the Prevention of Blindness. Essential Equipment List for Cataract Surgery. 2015.
- International Agency for the Prevention of Blindness. IAPB essential list for low vision services. 2017;(March):1–14.
- International Agency for the Prevention of Blindness. IAPB essential list for glaucoma. 2017;(March).
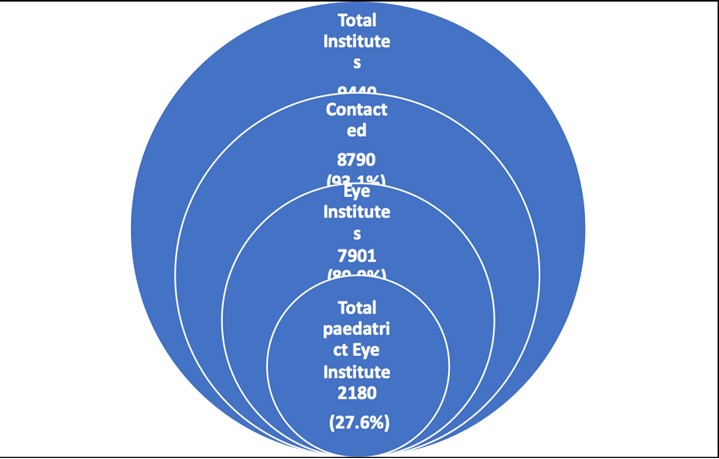
Figure 1: Proportion of eye institutes having paediatric oriented services out of total institutes.
Table 1: State-wise proportion of eye-institutes and paediatric eye institutes
| Sr. No. | State | Number of eye-institutes (N=7901) | Paediatric eye institutes (N=2180) | Proportion of paediatric eye institute out of all eye institutes (%) |
| 1 | Andhra Pradesh | 397 (5.0) | 68 (3.1) | 17.1 |
| 2 | Arunachal Prad | 8 (0.1) | 1 (0) | 12.5 |
| 3 | Assam | 101 (1.3) | 26 (1.2) | 25.7 |
| 4 | Bihar | 248 (3.1) | 57 (2.6) | 22.9 |
| 5 | Chattisgarh | 103 (1.3) | 29 (1.3) | 28.2 |
| 6 | Goa | 62 (0.8) | 7 (0.3) | 11.3 |
| 7 | Gujarat | 648 (8.2) | 206 (9.4) | 31.8 |
| 8 | Haryana | 329 (4.2) | 119 (5.5) | 36.2 |
| 9 | Himachal Pradesh | 62 (0.8) | 12 (0.6) | 19.4 |
| 10 | Jharkhand | 183 (2.3) | 51 (2.3) | 27.9 |
| 11 | Karnataka | 504 (6.4) | 127 (5.8) | 25.2 |
| 12 | Kerala | 219 (2.8) | 40 (1.8) | 18.3 |
| 13 | Madhya Pradesh | 242 (3.1) | 67 (3.1) | 27.7 |
| 14 | Maharashtra | 1360 (17.2) | 492 (22.6) | 36.2 |
| 15 | Manipur | 8 (0.1) | 2 (0.1) | 25.0 |
| 16 | Meghalaya | 14 (0.2) | 3 (0.1) | 21.4 |
| 17 | Mizoram | 11 (0.1) | 7 (0.3) | 63.6 |
| 18 | Nagaland | 9 (0.1) | 0 (0) | 0 |
| 19 | Odisha | 173 (2.2) | 27 (1.2) | 15.6 |
| 20 | Punjab | 324 (4.1) | 118 (5.4) | 36.4 |
| 21 | Rajasthan | 424 (5.4) | 112 (5.1) | 26.4 |
| 22 | Sikkim | 6 (0.1) | 1 (0.1) | 16.7 |
| 23 | Tamil Nadu | 499 (6.3) | 112 (5.1) | 22.4 |
| 24 | Telangana | 415 (5.3) | 50 (2.3) | 12.0 |
| 25 | Tripura | 14 (0.2) | 4 (0.2) | 28.6 |
| 26 | Uttar Pradesh | 718 (9.1) | 196 (8.9) | 27.3 |
| 27 | Uttarakhand | 99 (1.3) | 30 (1.4) | 30.3 |
| 28 | West Bengal | 377 (4.8) | 73 (3.3) | 19.4 |
Table 2: Proportion of eye-institutes in Union Territories
| Sr. No. | State | Number of Eye-Institutes (N=7901) | Paediatric Eye-Institutes (N=2180) | Proportion (%) |
| 1 | Andaman & Nicobar Islands | 1 (0) | 1 (0) | 100.0 |
| 2 | Chandigarh | 21 (0.3) | 10 (0.5) | 47.6 |
Leave a Comment