

 FP1422 : Orbital mass as presenting sign of underlying malignancy: Clinical, Pathological features & Outcomes
FP1422 : Orbital mass as presenting sign of underlying malignancy: Clinical, Pathological features & OutcomesDr. AKSHAY NAIR
Dr. S.NATARAJAN, Dr. NITA AMIT SHAH
Abstract
Purpose: To describe the clinical features and outcomes of patients presenting with orbital metastases as the first sign of underlying malignancy
Methods: Retrospective case series
Results: Between 2014-2019, 30 cases of orbital metastases were diagnosed, of which orbital metastases were the presenting feature in 10/30 (30%) cases. Lung was the most common site of primary tumour (4/10;40%) followed by breast (3/10;30%). Other sites were prostate, gall bladder and colon. Mean duration of complaints prior to presentation was 2.5 months (range:1-6 months). Mean number of metastatic sites (PET-CT screening) at time of diagnosis was 3.3 . All cases were treated with palliative chemo/radiotherapy; 8/10 (75%) patients died due to cancer-related causes while on treatment. Mean survival following diagnosis was 5.8 months.
Conclusion: Malignancies presenting primarily as orbital masses are rare. In our cohort, such cases had disseminated systemic metastases and were associated with poor survival
Full Text
Clinical features and outcomes in patients with orbital metastasis as the presenting sign of underlying malignancy: A case series.
Introduction:
Orbital metastatic tumours are relatively uncommon, and the clinical presentation and radiological features depend on the primary site. Tumours that metastasise to the orbit are estimated to account for up to 13% of all orbital tumours. [1-4] It has been reported that over the natural course of the disease, between 2-5% of all cancer patients may develop an orbital metastatic lesion.[5] The most common route for spread of the tumour from its primary origin to the orbit is the haematogenous route. The most common primary site is breast, followed by the lung and prostate.[4] Other uncommon sites include the kidneys, pancreas, cervix, thyroid, stomach and melanomas. [4-10] While most patients who present with orbital metastatic lesions have a pre-existing diagnosis of a primary tumour between 15-42% of patients, the orbital mass is the presenting sign of a previously undiagnosed tumour.[4,11,12] Common presenting features of orbital metastatic tumours include diplopia, pain, proptosis, reduced vision, ptosis and a palpable mass lesion.[1,5] The prognosis of orbital metastases has remained largely unchanged over the past few decades: Valenzuela et al. reported that survival was limited to 1.5 years after initial diagnosis, independent of the histological type; with 29% of patients in their cohort were alive after 17 months.[12] In this communication we present the clinical and the pathological features along with outcomes of patients in whom an orbital mass was the presenting feature of an underlying malignancy.
Methods:
This retrospective study was approved by the local institutional review board which waived informed consent. The report adhered to the ethical principles outlined in the Declaration of Helsinki as amended in 2013. The study cohort composed of all patients diagnosed with orbital metastatic tumours between 2014 and 2019. Data on lesion type and location, surgery performed, presenting complaints, histopathological diagnoses, comprehensive ophthalmic examination findings, clinical photographs, systemic history and Positron Emission Tomography – Computed Tomography (PET/CT) findings were collected and analyzed.
Results:
- Demographics:
In all 30 cases, orbital metastatic tumours were diagnosed. Of these, 20 (66.7%) cases had a previous diagnosis of a malignancy. 10/30 (33.3%) had no prior history of cancer. These ten patients in whom the orbital metastasis was the presenting feature of previously undiagnosed systemic malignancy was the primary analysis group. The mean follow-up was 7.8 months. All patients diagnosed as orbital metastatic tumour underwent a PET-CT scan, oncology consult and subsequent management as per the multidisciplinary tumour board’s recommendation. In these 10 cases, lung (4/10; 40%) was the most common primary site followed by breast (3/10; 30%). One case each of primary prostatic cancer, adenocarcinoma of the gall bladder and primary melanoma of the colon were noted. In this cohort, (6/10) 60% of the patients for female the mean age presentation was 68 years with a range of 52 – 77 years.
i Clinical features:
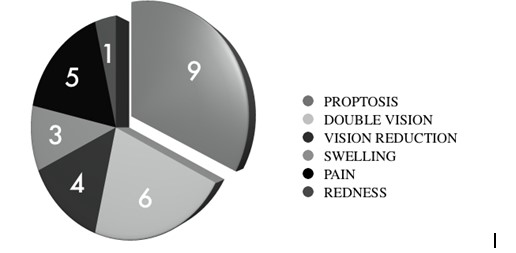
The most common presenting complaint was proptosis (90%) followed by diplopia (60%), ocular pain (50%), vision loss (40%) and mass lesion (30%). The mean duration from initial orbital symptom to the final diagnosis of an orbital metastatic tumour was 2.25 months (range: 1-6 months). As mentioned earlier, all patients underwent a systematic evaluation that included PET/CT scans. The mean number of metastatic sites involved at the time of diagnosis of the orbital lesion was 3.3. A detailed systemic history was elicited from all patients – it was observed that 7/10 (70%) of the patients had no systemic complaints related or attributable to their primary tumour. Lower back pain, constipation and severe headache were observed in one patient each and these symptoms were retrospectively attributable to their primary or metastatic tumours.
Management and Outcomes:
In terms of management, 8 out of 10 patients underwent an incision biopsy of the orbital mass. One patient underwent a PET/CT scan prior to orbital biopsy which was suspicious of a primary mass lesion in the abdomen. This was followed by an exploratory laparotomy which led to the diagnosis of a primary adenocarcinoma of the gall bladder and an FNAC of the orbital mass subsequently confirmed the diagnosis of orbital metastasis. One patient presented with vision reduction and was found to have a breast mass the patient underwent a PET/CT scan which showed orbital, brain and spinal metastatic lesions. All patients underwent multimodal management, based on the advice of a medical and radiation oncologists. All 10/10 patients received chemotherapy for the primary cancer additionally four patients underwent radiotherapy. Three (30%) patients also underwent surgery of the primary lesion, which was either to confirm the diagnosis of the primary tumour or palliative in nature.
Telephonic follow-up was carried out and it was noted that 8/10 (80%) of the patients had died due to disease and in this subset of patients whose death was attributable to the primary cancer, the mean duration from diagnosis of tumour to death was 5.8 months.
Discussion:
To the best of our knowledge this is the first series from India documenting the clinical features and outcomes of patients whom the orbital lesion was the presenting feature of a disseminated underlying malignancy. The clinical manifestations of orbital metastasis or fairly common and similar across all series. The patients typically present with sudden onset diplopia, reduced vision, visible or palpable lump beneath the eyelid or the orbital margin along with pain.[4,5,13] Clinical examination in these patients typically reveals proptosis and displacement of the globe with a palpable mass. The key features in these cases are the rapid onset and severity of symptoms which indicate a progressive and aggressive disease process. Additionally, pain and other inflammatory signs which would be suggestive of orbital inflammatory disease are absent.
El-Hadad and colleagues reported the multidisciplinary management of orbital metastasis and survival outcomes of 118 patients.[14] In their series, 22/118 (19%) patients presented with orbital metastasis as the first manifestation of metastatic cancer. They have mentioned that this is at the lower end of the spectrum of figures reported in literature mainly due to the fact that their study was from a comprehensive cancer care hospital where patients are more likely to have a diagnosis of cancer than in series generated from eye hospitals. Indeed, other studies have shown that in up to a third of all orbital metastatic tumours, the primary tumour remains unknown despite systemic evaluation and long follow-up.[4,13,15,16] However, in our series the final histopathological diagnosis was obtained in all cases.
In our series we found that the average number of metastatic sites that were identified on imaging was 3.3. This indicates that the underlying malignancy was fairly advanced and disseminated prior to diagnosis. In the series by El-Hadad and colleagues, they reported that 40% of all their patients with orbital metastasis had oligo metastatic disease. This meant that the orbit what is the only identifiable site of metastasis (in a patient with a previously treated cancer).[14]
Char and colleagues have reported that in their series, the median survival was 1.3 years amongst all patients of orbital metastasis and the two-year survival rate was 27%.[17] They also noted that there was no significant difference in survival duration between patients with and without a known primary tumour at the time the orbital metastasis was diagnosed. In contrast, our data showed that patients with orbital metastases and a previous diagnosed cancer at the time of presentation, the mean survival was 12.3 months. In contrast, the mean survival was only 5.8 months among those with no known primary. This difference was statistically significant (p<0.005); age and gender were not found to play any significant role in the overall survival. In both groups in our study, lung and breast were the most common primary sites.
It was noted in our series that 7 out of 10 patients did not report any systemic signs or symptoms that could be attributable to the primary tumour. It is likely that the patients were unaware or disregarded early warning symptoms. Surveys conducted to assess the level of awareness and knowledge about cancers and associated risk factors among households in India have shown that among many communities there is a very low level of awareness about warning signs and symptoms.[18] Poor awareness often leads to poor uptake of screening modalities and delay in seeking help for cancer like symptoms.[19]
In summary, we present our findings in patients who presented with an orbital mass as the first sign of an underlying disseminated malignancy which was previously undiagnosed. These patients were found to have aggressive disease; poorer prognosis with significantly shorter survival as compared to patients with orbital metastasis with a previous cancer diagnosis. Patients with complaints of recent onset proptosis, diplopia and orbital pain along with a palpable mass lesion should be treated with a high degree of suspicion for orbital metastatic tumours.
Legend:
Figure 1: A graphical representation of the clinical features of the patients.
Figure 2: External photograph of a 67-year-old male who presented with left sided sudden onset proptosis, diplopia, reduced vision and chemosis (Figure 2A). MRI showed a heterogeneous mass in the superomedial orbit displacing the globe downwards and outwards (Figures 2B, 2C). Contrast enhancement is seen and in the centre of the mass, a hyper intense focus is seen. An incisional biopsy confirmed the diagnosis of metastatic adenocarcinoma of the lung. The patient had secondaries in the liver and the orbit in addition to regional lymph node involvement.

References:
- Ahmad SM, Esmaeli B. Metastatic tumors of the orbit and ocular adnexa. Curr Opin Ophthalmol 2007;18:405-13.
- Magliozzi P, Strianese D, Bonavolontà P, Ferrara M, Ruggiero P, Carandente R, et al. Orbital metastases in Italy. Int J Ophthalmol 2015;8:1018-23.
- Bonavolontà G, Strianese D, Grassi P, Comune C, Tranfa F, Uccello G, et al. An analysis of 2,480 space-occupying lesions of the orbit from 1976 to 2011. Ophthalmic Plast Reconstr Surg 2013;29:79-86.
- Allen RC. Orbital metastases: When to suspect? When to biopsy?. Middle East Afr J Ophthalmol 2018;25:60-4.
- Matlach J, Nowak J, Göbel W. Papilledema of unknown cause. Ophthalmologe 2013;110:543-5
- Barajas-Ochoa Z, Suero-ABreu GA, Barajas-Ochoa A. Orbit and sinonasal metastasis as presenting sign of renal cell carcinoma. BMJ Case Rep . 2021;14(4):e240588.
- Pecen PE, Ramey NA, Richard MJ, Bhatti MT. Metastatic pancreatic carcinoma to the orbital apex presenting as a superior divisional third cranial nerve palsy. Clin Ophthalmol. 2012;6:1941-3.
- Mendia A, Shah CP, Grajo JR, Yachnis A, Yeung A, Cardenas-Goicoechea J, Murphy M. Orbital metastasis of squamous cell cervical cancer: A case report and review of literature. Gynecol Oncol Rep. 2020;35:100689.
- Ruiz JB, Orré M, Cazeau AL, Henriques de Figueiredo B, Godbert Y. 8F-DOPA PET/CT in Orbital Metastasis From Medullary Thyroid Carcinoma. Clin Nucl Med. 2016;41(6):e296-7.
- Brundridge WL, Heymann HB, Spengler A, DeBacker CM, Holck DEE. Gastrointestinal stromal tumor metastatic to the orbit. Orbit. 2021. doi: 10.1080/01676830.2021.1914671.
- Montejano-Milner R, López-Gaona A, Fernández-Pérez P, Sánchez-Orgaz M, Romero-Martín R, Arbizu-Duralde A. Orbital metastasis: Clinical presentation and survival in a series of 11 cases. Arch Soc Esp Oftalmol (Engl Ed). 2020;S0365-6691(20)30317-8.
- Valenzuela AA, Archibald CW, Fleming B, Ong L, O’Donnell B, Crompton JJ, et al. Orbital metastasis: Clinical features, management and outcome. Orbit 2009;28:153-9.
- Shields JA, Shields CL, Brotman HK, Carvalhi C, Perez N, Eagle Jr RC. Cancer Metastatic to the Orbit: The 2000 Robert M. Curts Lecture. Ophthalmic Plast Reconstr Surg . 2001;17(5):346-54.
- El-Hadad C, Koka K, Dong W, Do T, Haider M, Ursua JD, Ning J, Debnam JM, Esmaeli B. Multidisciplinary Management of Orbital Metastasis and Survival Outcomes. Ophthalmic Plast Reconstr Surg. 2021. doi: 10.1097/IOP.0000000000001939
- Ng E, Ilsen PF. Orbital metastases. Optometry. 2010; 81(12):647-57.
- Magliozzi P, Strianese D, Bonavolontà P, Ferrara M et al. Orbital Metastases in Italy. Int J Ophthalmol. 2015; 8(5): 1018–1023.
- Char D, Miller T, Kroll S. Orbital metastases: diagnosis and course. Br J Ophthalmol. 1997; 81(5): 386–390.
- Raj S, Piang LK, Nair KS, Tiwari VK et al. Awareness regarding risk factors, symptoms and treatment facilities for cancer in selected states of India. Asian Pac J Cancer Prev. 2012;13(8):4057-62.
- Sahu DP, Subba SH, Giri PP. Cancer awareness and attitude towards cancer screening in India: A narrative review. J Family Med Prim Care. 2020;9(5):2214-2218.
Leave a Comment